
The earliest sign of the heart is the appearance of paired endothelial strands-angioblastic cords-in the cardiogenic mesoderm during the third week .An inductive influence from the anterior endoderm stimulates early formation of the heart. These cords canalize to form thin heart tubes.

As lateral embryonic folding occurs, the endocardial tubes approach each other and fuse to form a heart tube.Fusion of the heart tubes begins at the cranial end of the developing heart and extends caudally.

The heart begins to beat at 22 to 23 days Blood flow begins during the fourth week and can be visualized by Doppler ultrasonography






The fusion begins at the cranial ends of the heart tubes and extends caudally until a single tubular heart is formed. The endothelium of the heart tube forms the endocardium of the heart. As the heart elongates, it forms regional segments and bends upon itself, giving rise to an S-shaped heart










.png)
COMMON TYPES OF PERSISTENT TRUNCUS ARTERIOSUS (PTA)
Diagram of a malformed heart illustrating transposition of the great arteries (TGA). The ventricular and atrial septal defects allow mixing of the arterial and venous blood. TGA is the most common single cause of cyanotic heart disease in newborn infants. As here, it is often associated with other cardiac anomalies (ventricular septal defect [VSD] and atrial septal defect [ASD]).

TETRALOGY OF FALLOT. Observe the four cardiac deformities of this tetralogy: pulmonary valve stenosis, ventricular septal defect (VSD), overriding aorta, and hypertrophy of the right ventricle.

Sagittal sections of the primordial heart during the fourth and fifth weeks illustrating blood flow through the heart and division of the atrioventricular canal. The arrows are passing through the sinuatrial (SA) orifice. D, Coronal section of the heart at the plane shown in C. Note that the interatrial and interventricular septa have started to develop.



















Ultrasound scan of a fetal heart at 23.4 weeks' gestation with an atrioventricular septal defect and a large ventricular septal defect (VSD).




Postductal coarctation of the aorta. B, Diagrammatic representation of the common routes of collateral circulation that develop in association with postductal coarctation of the aorta. C and D, Preductal coarctation.


Closure of the ductus arteriosus (DA). A, The DA of a newborn infant. B, Abnormal patent DA in a 6-month-old infant. C, The ligamentum arteriosum in a 6-month-old infant.


Pharyngeal and pharyngeal arch arteries. A, Left side of an embryo (approximately 26 days). B, Schematic drawing of this embryo showing the left pharyngeal arch arteries arising from the aortic sac, running through the pharyngeal arches, and terminating in the left dorsal aorta. C, An embryo (approximately 37 days) showing the single dorsal aorta and that most of the first two pairs of pharyngeal arch arteries have degenerated





The relation of the recurrent laryngeal nerves to the pharyngeal arch arteries. A, At 6 weeks, showing the recurrent laryngeal nerves hooked around the sixth pair of pharyngeal arch arteries. B, At 8 weeks, showing the right recurrent laryngeal nerve hooked around the right subclavian artery and the left recurrent laryngeal nerve hooked around the ductus arteriosus and the arch of the aorta. C, After birth, showing the left recurrent nerve hooked around the ligamentum arteriosum and the arch of the aorta.


FETAL CIRCULATION

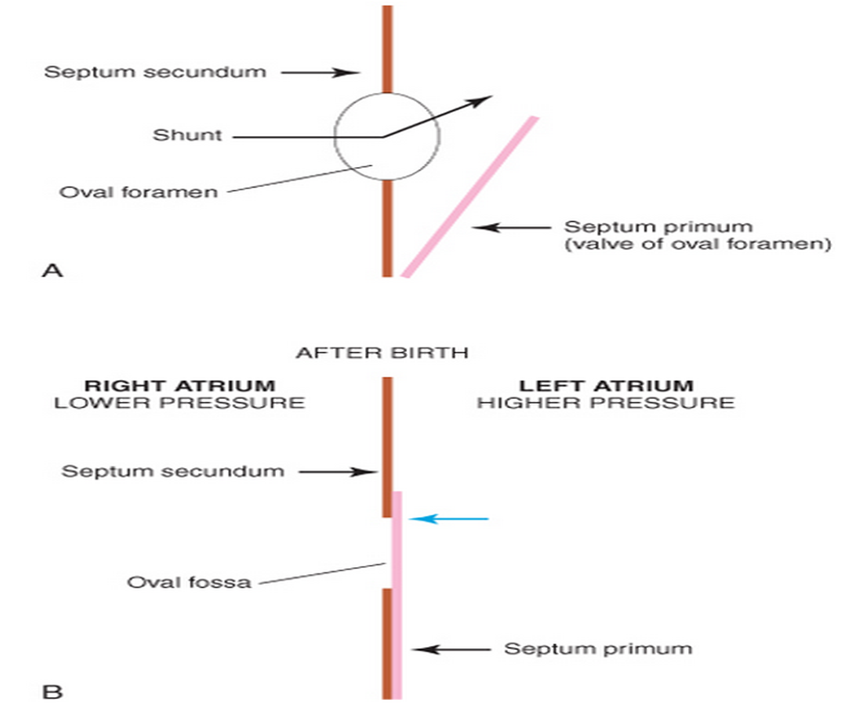
Observe that three shunts permit most of the blood to bypass the liver and lungs: (1) ductus venosus, (2) oval foramen, and (3) ductus arteriosus.

Hiç yorum yok:
Yorum Gönder